
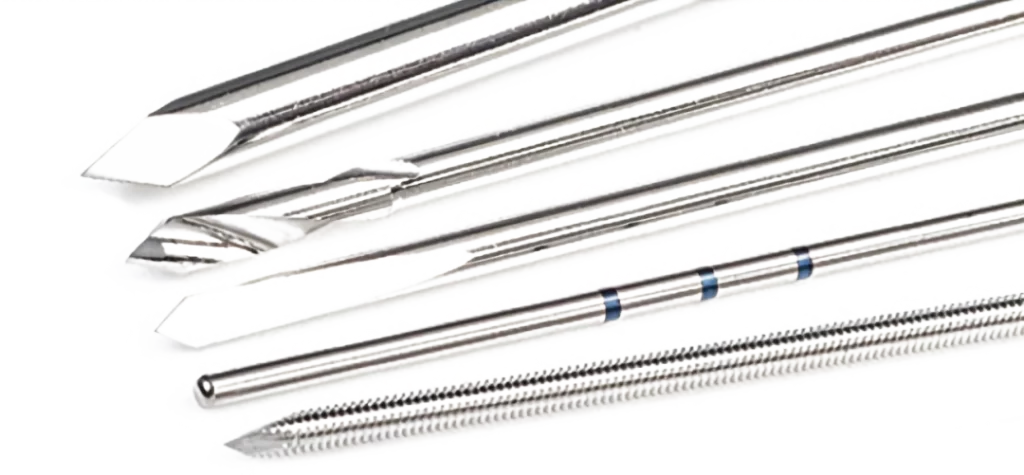
Kirschner wires or K wires are metallic wire (stainless steel) sharpened one or both side, are used to hold bone fragments together (pin fixation) or to provide an anchor for skeletal traction.
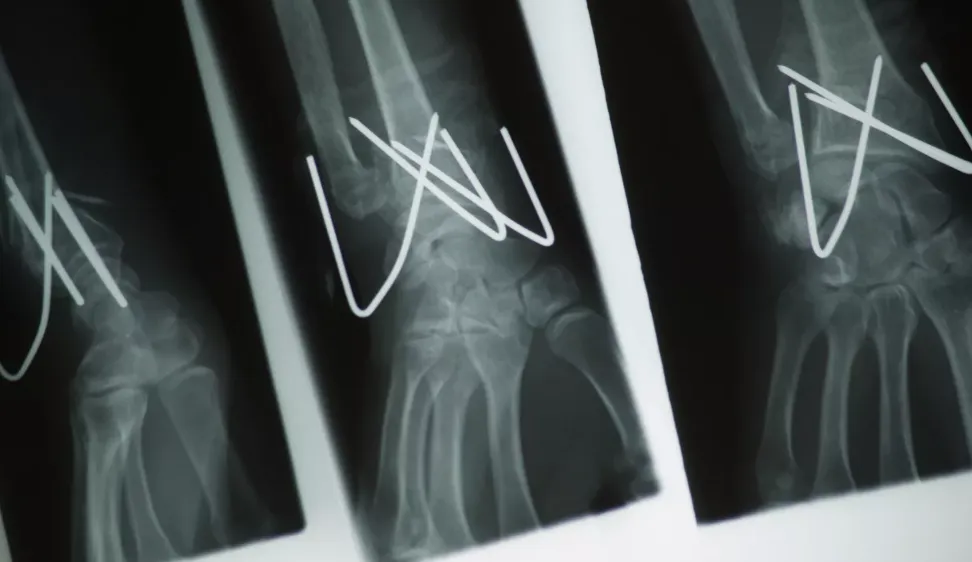
K wire (Kirschner wire) is now widely used in orthopedics and other types of surgery. These wires can be drilled through the bone to hold the fragments in place. They can be placed percutaneously (through the skin) or can be buried beneath the skin.
K-wires are often used to stabilize a broken bone and can be removed in the office once the fracture has healed. Some K-wires are threaded, which helps prevent movement or backing out of the wire, although that can also make them more difficult to remove.
K Wires (KirschnerWires) are available in various Types, lengths and diameters.
Types: Single Trocar, Double Trocar, Fully Threaded
Diameters: 0.8mm, 1mm, 1.2mm, 1.4mm, 1.5mm, 1.6mm, 1.8mm, 2mm. 2.2mm, 2.3mm, 2.5mm, 3mm
Lengths: 80mm, 100mm, 125mm, 150mm, 175mm, 200mm, 225mm, 250mm
K Wire (Kirschner Wire) Indications for Use
K Wire (Kirschner Wire) is indicated for use in the fixation of bone fractures, bone reconstruction, and as guide pins for insertion of other implant. The size of the Pin chosen should be adapted to the specific indication. Surgeon judgement is required to ensure a K Wire (Kirschner Wire) is appropriate for the indication.
K Wires (Kirschner Wires) are indicated for use in the following conditions:
K Wires (Kirschner Wires) are used for temporary fixation during some operations. After definitive fixation they are then removed.The pins are usually removed four to five weeks post operation.
They can be used for definitive fixation if the fracture fragments are small. In some settings they can be used for intramedullary fixation of bones such as the ulna.
Tension band wiring is a technique in which the bone fragments are transfixed by K-wires which are then also used as an anchor for a loop of flexible wire. As the loop is tightened the bone fragments are compressed together. Fractures of the kneecap and the olecranon process of the elbow are commonly treated by this method.
K Wire (Kirschner Wire) is passed through the skin then transversely through the bone and out the other side of the limb. The wire is then attached to some form of traction so that the pull is applied directly to bone. In traction of the femur for example, the protruding ends of the wire are fixed to the legs of a horsehoe shaped frame which maintains tension in the wire while the crook of the horseshoe is attached via line and pulleys to weights which maintain the traction.
K Wire (Kirschner Wire) can be used to guide cannulated screws to a precise location.
K Wire (Kirschner Wire) General principles
K Wire (Kirschner Wire) size is chosen according to the age of the child and the size of the fragment.
The entry point, together with the correct direction of the K-wire, is the key to optimal fixation.
For most simple fractures, two, occasionally three, K Wires (Kirschner Wires) give sufficient stabilization if the K-wires:
Are of the correct size (1.6/2.0 mm)
Do not cross each other at the fracture level
Are intraosseous
K Wire (Kirschner Wire) osteosynthesis usually requires additional plaster cast protection.
Advantages:
Cheap,Universally available,Can be inserted by hand (with a T-handle), but also with a drill provided thermal injury is avoided
Disadvantages:
Not functionally stable,Size of K Wire (Kirschner Wire)
The following points influence the size of the K Wire (Kirschner Wire)
Patient age/weight
- In children younger than 5–6 years, 1.6 mm K Wires (Kirschner Wires) are used for fractures around the shoulder, elbow, knee, and ankle joints.
- In children above this age, 2.0 mm K Wires (Kirschner Wires) are usually used.
- It is important to consider the weight of the patient when choosing the diameter of the K-wire.
Fracture location
- Metaphyseal fractures of the long bones require at least 1.6 mm K-wires (Kirschner Wires). If only two wires are used, larger diameter wires may be necessary.
- Fractures of small bones (hand and foot) require 1.0 – 1.6 mm K-wire.
Fragment size
The size of the K Wire (Kirschner Wire) should be chosen according to the size of the fragment. For example, a fracture of the medial epicondyle of the humerus requires a K-wire of smaller diameter than a fracture of the lateral humeral condyle.
K Wire (Kirschner Wire) trajectory
For fractures fixed with two (or three) K Wires (Kirschner Wires) from only one side, one size larger K-wires are used than for bilateral crossed K-wiring.
For example, for bilateral crossed K-wiring of a supracondylar humeral fracture, 1.6 mm K-wires can be used, whereas for radial divergent wiring of the same fracture, 2.0 mm K-wires are preferable.
K Wire (Kirschner Wire) Planning,K Wire (Kirschner Wire) entry point
K Wires (Kirschner Wires) are, in most cases, inserted from the free fragment into the main fragment. This allows the K-wire to be used as a joystick for manipulating the free fragment.
The entry points of the K Wires (Kirschner Wires) should be chosen so that they are as far apart as possible where they cross the fracture line. This guarantees maximal rotational stability.
The choice of the entry point must correlate with the planned direction of the K-wires and the end fixation point in the main fragment.
Ideally, if the anatomical site permits, the K Wires (Kirschner Wires) should be introduced as perpendicular as possible to the fracture plane. In certain sites, this is not achievable and mechanical stability should not be compromised by obsessive adherence to the above principle.
K Wire (Kirschner Wire) direction in transverse
The direction of the K Wires (Kirschner Wires) should be chosen so that the K-wires are well separated at the fracture level.
To achieve this, the length of the fracture line is divided into four equal parts. Ideally, when using two K-wires, the wires should pass approximately through the green areas in the illustration.
Monolateral divergent K Wires (Kirschner Wires)
For oblique (>30°) metaphyseal fractures crossed K Wire (Kirschner Wire) fixation may be very difficult, or impossible, as at least one of the K Wires (Kirschner Wires) will run nearly parallel to the fracture line.
For oblique fractures, therefore, divergent monolateral K-wire fixation is more suitable. For this technique, one size larger K Wires (Kirschner Wires) should be used than for cross K-wiring.
If lateral divergent K Wire (Kirschner Wire) fixation is not possible, for example, due to soft tissue condition or a structure at risk, another stabilization technique should be used (eg, external fixator or plate).
Stab incision
A small incision or a direct puncture with the K-wire is made over the planned entry point. An incision is recommended to avoid skin damage, which might cause pin-track infection.
K Wire (Kirschner Wire) insertion
To avoid thermal injury, especially to the physis, K Wires (Kirschner Wires) should be inserted by hand or using an oscillating drill.
If a standard drill is used, it must be run as slowly as possible to avoid a thermal effect.
Additionally, irrigate the K Wire (Kirschner Wire) during drilling with a cooled irrigation fluid.
If a drill is used, the K Wire (Kirschner Wire) is initially inserted manually through the skin incision, onto the chosen bony entry point. While maintaining the correct position of the tip, the drill is attached to the wire.
To prevent bending of the K Wire (Kirschner Wire), it can be helpful to insert the K-wire using an appropriate drill sleeve – this steadies the wire, protects the soft tissues, and ensures optimal direction.
It is helpful to reduce the length of the K Wire (Kirschner Wire) protruding from the drill to avoid whipping of the wire and loss of trajectory.
To avoid skidding, the K Wire (Kirschner Wire) tip should initially be held as orthogonal as possible to the bone surface until the tip of the wire has a good purchase.
Once the tip of the K Wire (Kirschner Wire) has obtained a good purchase, the angulation of the K-wire should be corrected according to the planned direction of the K-wire.
As soon as increased resistance is felt, check that the tip of the K Wire (Kirschner Wire) is engaged in the far cortex of the main fragment.
The tip of the K-wire should penetrate the whole depth of the far cortex, but not protrude more than 2–3 mm. This is to avoid neurovascular damage and soft tissue irritation.
The free end of the wire is usually left protruding through the skin and is bent through 180°. A sterile dressing protects the entry wound around the wire.
No more than two attempts should be made to insert any one wire across a physis. Repeated puncture of the physis by multiple attempts to insert the wire can result in subsequent growth disturbance.
K Wire (Kirschner Wire) removal
The timing of K Wire (Kirschner Wire) removal is a matter of judgment by the treating surgeon, based on the age of the child, the pattern of the injury, as well as additional injuries.
Depending on the age of the child, fracture healing has reached the stage where redisplacement is highly unlikely after 3–4 weeks and the K-wires can be removed.
K Wire (Kirschner Wire) Contraindications
Contraindications may be qualified or total, and need to be taken into consideration when evaluating the prognosis in each case. The physician’s education, training and professional judgement must be relied upon to choose the most appropriate device and treatment. Conditions presenting an increased risk of failure include:
- Any active or suspected latent infection or marked local inflammation in or about the affected area.
- Compromised vascularity that would inhibit adequate blood supply to the fracture or the operative site.
- Bone stock compromised by disease, infection or prior implantation that can not provide adequate support and/or fixation of the devices.
- Material sensitivity, documented or suspected.
- Obesity. An overweight or obese patient can produce loads on the implant that can lead to failure of the fixation of the device or to failure of the device itself.
- Patients having inadequate tissue coverage over the operative site.
- Implant utilization that would interfere with anatomical structures or physiological performance.
- Any mental or neuromuscular disorder which would create an unacceptable risk of fixation failure or complications in postoperative care.
- Other medical or surgical conditions which would preclude the potential benefit of surgery.
- All associated diseases which could endanger the function and success of the K Wire (Kirschner Wire).
Warnings and Precautionary for K Wire (Kirschner Wire)
Before using K Wire (Kirschner Wire), the surgeon and ancillary staff should study the safety information in these instructions, as well as any product-specific information in the product description, surgical procedures and/or brochures.
wire is made from medical grade materials and are designed, constructed and produced with utmost care. These quality wire assure best working results provided they are used in the proper manner. Therefore, the following instructions for use and safety recommendations must be observed.
Improper use of wire can lead to damage to the tissue, premature wear, destruction of the instruments and injury to the operator, patients or other persons.
It is vital for the operating surgeon to take an active role in the medical management of their patients. The surgeon should thoroughly understand all aspects of the surgical procedure and instruments including their limitations. Care in appropriate selection and proper use of surgicalinstruments is the responsibility of the surgeon and the surgical team. Adequate surgical training should be completed before use of implants.
Factors which could impair the success of the operation:
- Allergies to implanted materials.
- Localized bone tumours.
- Osteoporosis or osteomalacia.
- System disease and metabolic disturbances.
- Alcohol and drug abuse.
- Physical activities involving excessive shocks, whereby the implant is exposed to blows and/or excessive loading.
- Patients who are mentally unable to understand and comply with the doctor’s instructions.
Poor general health.
The following adverse effects are the most common resulting from implantation:
- Loosening of the wire, which may result from cyclic loading of the fixation site and/or tissue reaction of the implant.
- Early and late infection.
- Further bone fracture resulting from unusual stress or weakened bone substance.
- Temporary or chronic neural damage resulting from pressure or hematomata.
- Wound hematomas and delayed wound healing.
- Vascular disease including venal thrombosis, pulmonary embolism and cardiac arrest.
- Heterotopic ossification.
- Pain and discomfort due to presence of the K Wire (Kirschner Wire).
- Mechanical failure of the implant, including bending, loosening or breakage.
- Migration of implant resulting in injury.
Preoperative Planning for K Wire (Kirschner Wire)
The operating planning is carried out following a thorough clinical evaluation of the patient, Also, x-rays must be taken to allow a clear indication of the bony anatomy and associated deformities. At the time of the operation, the corresponding implantationinstruments in addition to a complete size of K Wire (Kirschner Wire) must be available.
The clinician should discuss with the patient the possible risks and complications associated with the use of implants. It is important to determine pre-operatively whether the patient is allergic to any of the implant materials. Also, the patient needs to be informed that the performance of the device cannot be guaranteed as complications can affect the life expectancy of the device.
K Wire (Kirschner Wire) Precautions
- Confirm functionality of instruments and check for wear during reprocessing. Replace worn or damaged instruments prior to use.
- It is recommended to use the instruments identified for this wire.
- Handle devices with care and dispose worn bone cutting instruments in a sharps container.
- Always irrigate and apply suction for removal of debris potentially generated during implantation or removal.
K Wire (Kirschner Wire) Warnings
K Wire (Kirschner Wire) can break during use (when subjected to excessive forces). While the surgeon must make the final decision on removal of the broken part based on associated risk in doing so, we recommend that whenever possible and practical for the individual patient, the broken part should be removed. Be aware that implants are not as strong as native bone. Implants subjected to substantial loads may fail.
Instruments, screws and cut plates may have sharp edges or moving joints that may pinch or tear user’s glove or skin.
Take care to remove all fragments that are not fixated during the surgery.
While the surgeon must make the final decision on implant removal, we recommend that whenever possible and practical for the individual patient, fixation devices should be removed once their service as an aid to healing is accomplished. wire removal should be followed by adequate post-operative management to avoid refracture.
K Wire (Kirschner Wire) General Adverse Events
As with all major surgical procedures, risks, side effects and adverse events can occur. While many possible reactions may occur, some of the most common include: Problems resulting from anesthesia and patient positioning (e.g. nausea, vomiting, dental injuries, neurological impairments, etc.), thrombosis, embolism, infection, nerve and/or tooth root damage or injury of other critical structures including blood vessels, excessive bleeding, damage to soft tissues incl. swelling, abnormal scar formation, functional impairment of the musculoskeletal system, pain, discomfort or abnormal sensation due to the presence of the device, allergy or hypersensitivity reactions, side effects associated with hardware prominence, loosening, bending, or breakage of the device, mal-union, non-union or delayed union which may lead to breakage of the K Wire (Kirschner Wire), reoperation.


